Vitamin D is rarely recommended on its own anymore. The common instruction is to pair it with vitamin K2, on a specific rationale: vitamin D raises calcium levels, and without K2 to direct that calcium into bone, it is said to deposit in your arteries instead. Taken alone, according to this framing, vitamin D is not just ineffective but actively dangerous to your cardiovascular system.
That warning rests on a mechanism specific enough to test directly, which is unusual for a supplement claim. Most stay vague enough to avoid falsification. This one was put to randomized, placebo-controlled trials, with arterial calcium scored on CT scans before and after supplementation.
The trials reported their results, but they do not agree with each other.
So what does the evidence actually show about K2 and arterial calcification, and did a trial published in 2026 change the answer?
How Vitamin K Switches the Guard On
The mechanism behind the warning is real, and worth understanding before deciding what it does and doesn't prove.
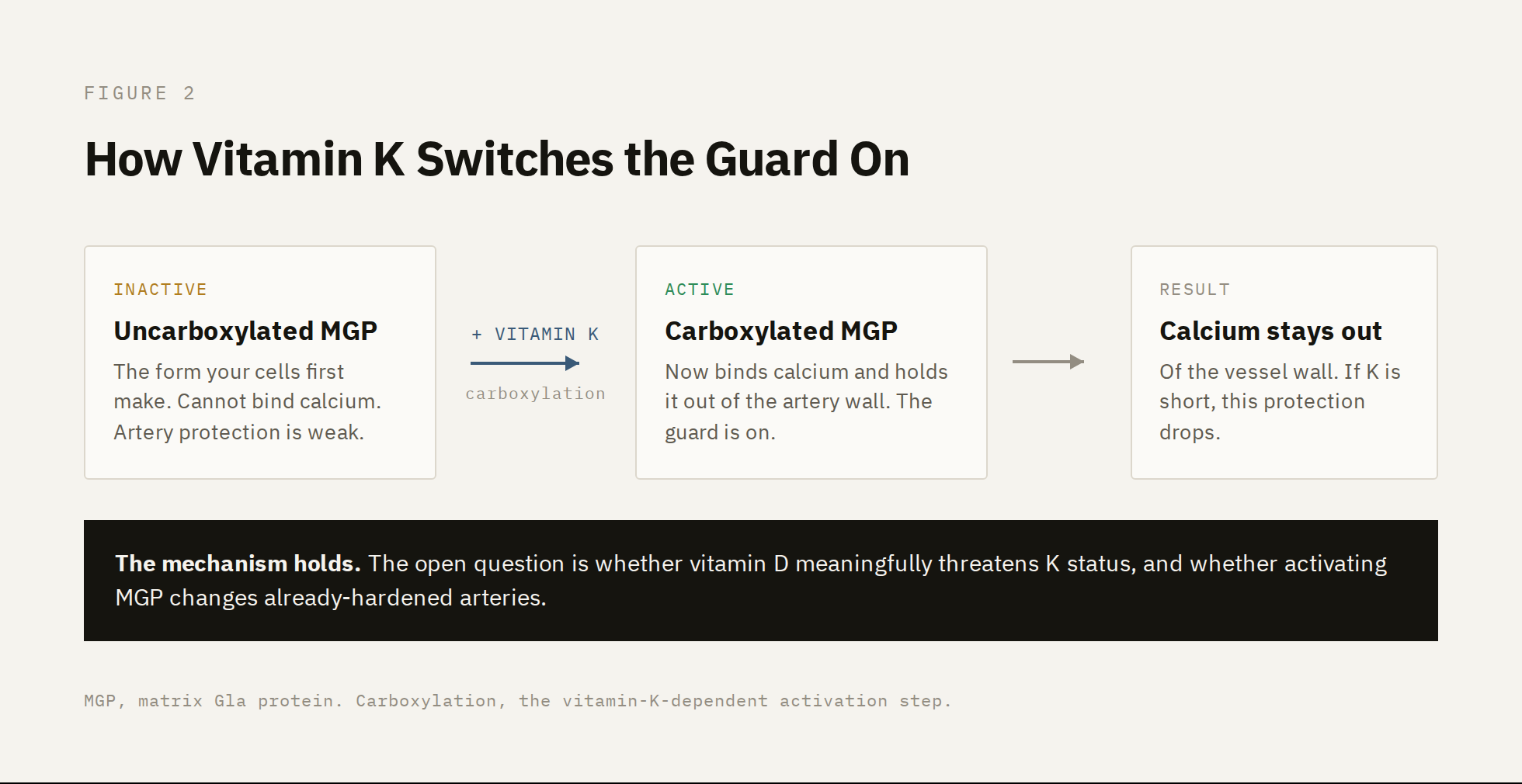
Your body produces a protein called matrix Gla protein, or MGP. Its job is to bind calcium in soft tissue, including the walls of your arteries, and keep it from forming mineral deposits. MGP is one of the main reasons circulating calcium does not simply settle into your blood vessels by default.
But MGP does not work in the form your cells first make it. It has to be switched on, through a chemical modification called carboxylation, and that step requires vitamin K. Without enough vitamin K, MGP stays in its uncarboxylated, largely inactive state, and its ability to hold calcium out of the artery wall drops.¹ Low vitamin K status, measured as a rise in uncarboxylated MGP, is associated with greater arterial calcification.¹
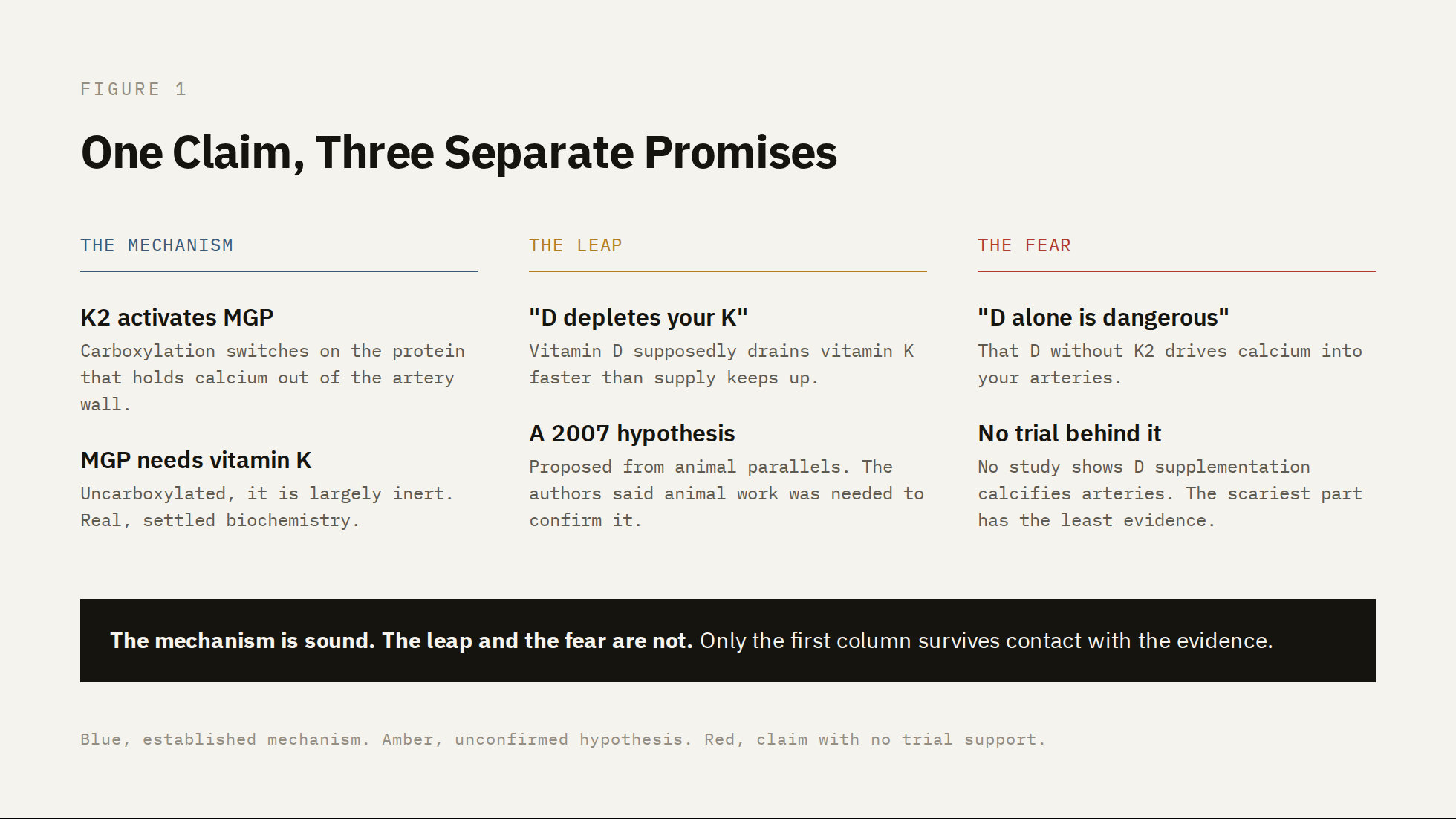
So the logic of the claim holds together at the level of mechanism. Vitamin K activates the protein that protects arteries from calcium. If you were short on vitamin K, you would expect that protection to weaken.
The problem is the next step, the one that the marketing adds. The popular version says that taking vitamin D actively drains your vitamin K, by raising demand for vitamin K-dependent proteins faster than your supply can keep up, which is what supposedly makes high-dose vitamin D dangerous on its own. That idea has a specific origin. It was published in 2007, in a journal called Medical Hypotheses, as an explicit hypothesis built mostly on similarities between vitamin D toxicity and vitamin K deficiency in animals.³ The paper proposed the model and stated plainly that animal experiments would be needed to confirm it.
A plausible mechanism and an unconfirmed hypothesis are two different things. The first describes how vitamin K protects arteries. The second is a specific, untested claim about vitamin D causing harm. The way to tell them apart is to look at what happens when the claim is actually tested in people.
What the Calcification Trials Measured
Three randomized controlled trials have tested whether vitamin K2 affects arterial or valvular calcification. Reading them in order shows why the question is not as settled as either side claims.
The first major trial was published in Circulation in 2022.⁴ Researchers enrolled 365 older men, average age 71, all with an aortic valve calcification score above 300 Agatston units, meaning established calcific disease. They received either 720 micrograms of MK-7 plus vitamin D daily or a placebo, for two years, with valve calcium scored on CT before and after. The supplement did what its biochemistry predicts at the molecular level. It improved vitamin K status, lowering uncarboxylated MGP, the same inactive protein from the mechanism above. It did not change the outcome. Valve calcification advanced by 275 units in the treatment group and 292 in the placebo group, a difference of 17 units with a confidence interval that crossed zero.⁴ The protein moved, but the calcium did not.
The second trial, the Valkyrie study, appeared in the Journal of the American Society of Nephrology in 2020.⁵ It studied 132 hemodialysis patients with atrial fibrillation, among the most heavily calcified patients in medicine, using a high dose of vitamin K2, 2000 micrograms. The result repeated the pattern. Vitamin K status improved, but calcium scores in the coronary arteries, the thoracic aorta, and the heart valves were no different across treatment arms.⁵ A higher dose, a higher-risk population, and the same disconnect between the marker and the artery.
After these two trials, the reasonable conclusion was that vitamin K2 corrects the underlying biochemistry without changing what happens in already-calcified arteries. A third trial was just published that complicated it.
VitaK-CAC was published in JAMA Cardiology in 2026.⁶ Its design differed in one decisive way. Instead of advanced valve disease or dialysis patients, it enrolled 180 people with symptomatic coronary artery disease and a coronary calcium score between 50 and 400 units, a milder and earlier stage of calcification. They received 360 micrograms of MK-7 or placebo for two years. This time the calcium scores diverged. Coronary calcification progressed more slowly in the MK-7 group than in the placebo group, and the difference reached statistical significance after adjustment for other factors.⁶
That is a genuinely positive result, and it deserves the same scrutiny applied to the null ones. The benefit was measured on a CT scan, not on heart attacks or deaths, which the trial did not assess. The authors were specific about the limit of their finding, noting that its clinical significance for plaque stability remains to be determined.⁶ What the trial showed is that vitamin K2 slowed the conversion of soft, noncalcified plaque into calcified plaque. Whether that slowing translates into fewer cardiovascular events is unknown.

It Isn't Whether K2 Works. It's When.
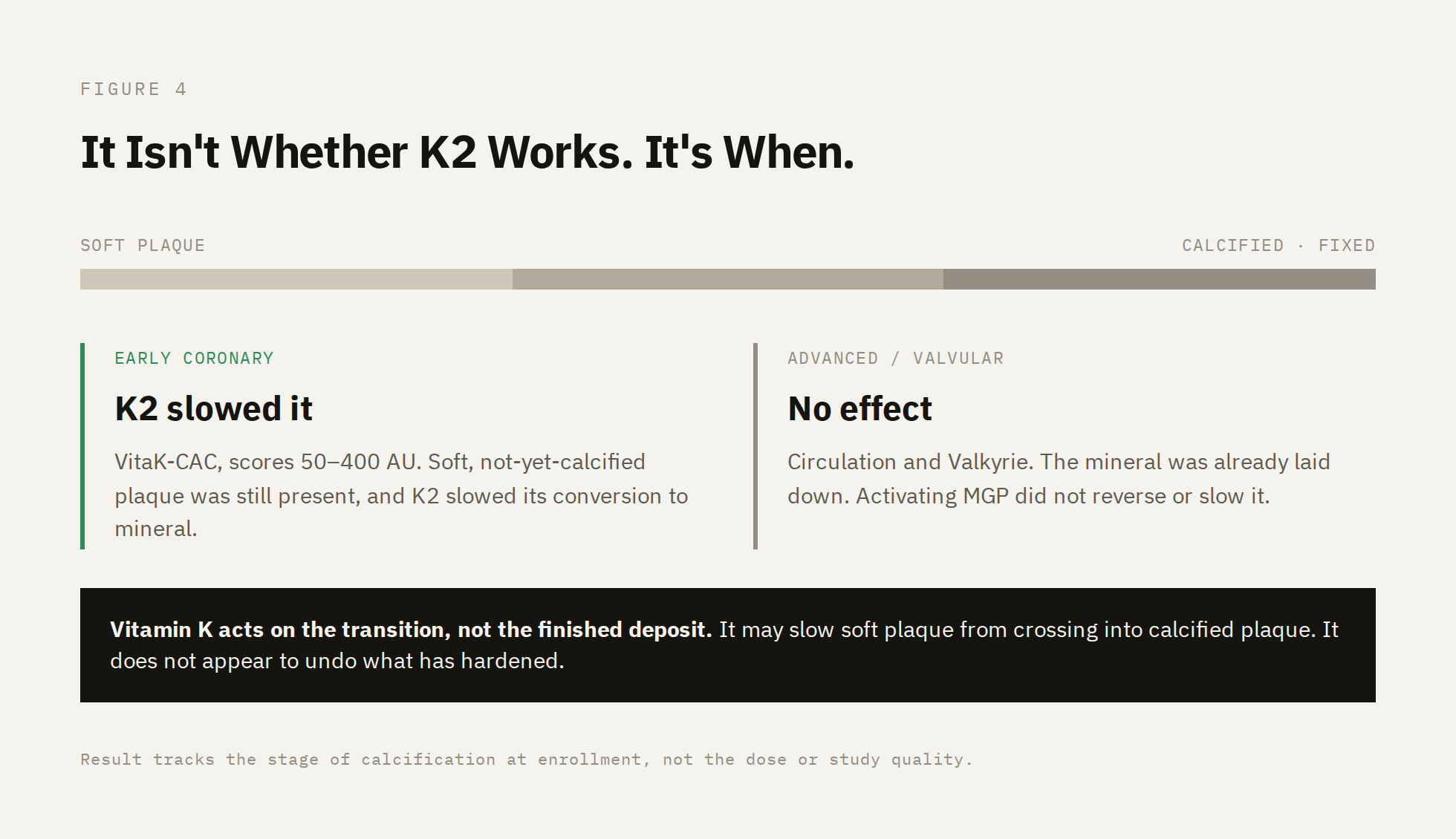
Set the three trials side by side and the contradiction starts to resolve. The variable that separates them is not dose, and it is not study quality. It is the stage of calcification in the people enrolled.
The two trials that found nothing studied advanced, established disease. Aortic valves already scored above 300 units in the Circulation trial.⁴ Dialysis patients in Valkyrie carried some of the heaviest calcification in clinical medicine.⁵ In both, the mineral was already laid down. The trial that found a benefit studied earlier disease, coronary scores between 50 and 400 units, with a measurable population of soft plaques that had not yet calcified.⁶ And the benefit it found was specific to those soft plaques, slowing their conversion into calcified ones.⁶
This points to a different model of what vitamin K is doing. Calcification is not a single event. It begins as soft, lipid-rich plaque and progresses, in some people, toward a hardened mineral state. Vitamin K, through activated MGP, appears to act on that transition. It may slow soft plaque from crossing over into calcified plaque. It does not appear to reverse or even slow calcification that has already formed, which is what the two null trials were asking it to do.
That reframing is consistent with more than these three studies. The team behind the 2026 trial noted that vitamin K had already shown calcification benefits in people with diabetes and end-stage kidney disease,⁶ conditions where the relevant question is ongoing progression rather than reversal of fixed disease. The pattern across the literature is not random noise. It tracks the biology of when, in the long arc of arterial calcification, the intervention is applied.
This is the question almost no coverage of vitamin K2 asks. The debate is framed as whether K2 protects your arteries, a yes or no answer the trials seem to contradict. The better question is when it might, and for whom. A 70-year-old with a calcified aortic valve and a 55-year-old with early, mostly soft coronary plaque are not the same case, and the evidence no longer suggests they should expect the same result.
What the Evidence Actually Supports
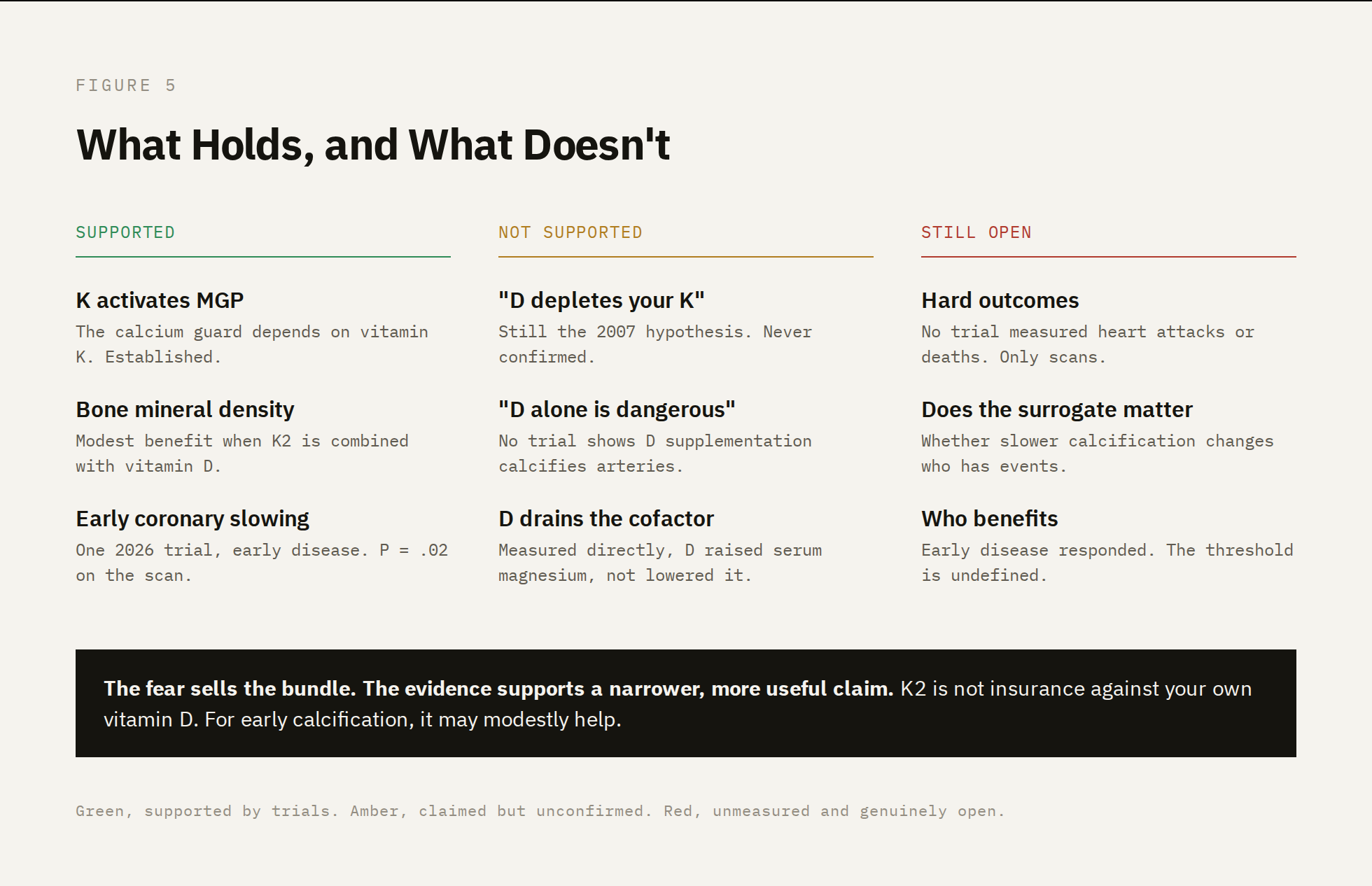
Start with what holds up. Vitamin K activates matrix Gla protein, and matrix Gla protein keeps calcium out of the artery wall.¹ Vitamin K2 has a modest benefit for bone mineral density when combined with vitamin D.⁹ And as of 2026, one well-designed trial supports a modest arterial benefit, slower coronary calcification in people with early, symptomatic coronary disease.⁶ A reader paying attention to the evidence should update toward taking vitamin K2 more seriously than the two earlier null trials alone would suggest.
Now what does not hold up. The specific claim that started this, that vitamin D taken without K2 is dangerous and drives calcium into your arteries, has no trial behind it. No study has shown that vitamin D supplementation causes arterial calcification. The mechanism proposed for that harm, vitamin D depleting your vitamin K, remains the 2007 hypothesis it began as.³ And the one trial that directly measured what vitamin D does to a mineral cofactor found the opposite of depletion. Six months of vitamin D raised serum magnesium rather than lowering it.¹⁰ The frightening half of the popular claim is the half with the least evidence under it.
So the honest position is narrower than either marketing or skepticism would have it. Taking higher amounts of vitamin K2 than you would get from food is not insurance against your own vitamin D, because vitamin D is not threatening your arteries to begin with. But K2 is also not inert. For someone with early coronary calcification, the newest evidence suggests it may slow the disease modestly, which is a more specific and more useful claim than the blanket one used by everyone on the internet.
What no trial has yet shown is the part that actually matters. Every study here measured calcium on a scan. None measured whether moving that number changes how many people have heart attacks or die. Slower calcification is a reasonable surrogate, but it is not the outcome. Until a trial follows hard endpoints rather than CT scores, the most important question about vitamin K2 and the heart remains exactly where it has been the whole time. Open.
References
1. Boxma PY, van den Berg E, Geleijnse JM, et al. Vitamin K intake and plasma desphospho-uncarboxylated matrix Gla-protein levels in kidney transplant recipients. PLoS One. 2012;7(10):e47991. doi:10.1371/journal.pone.0047991
2. Masterjohn C. Vitamin D toxicity redefined: vitamin K and the molecular mechanism. Med Hypotheses. 2007;68(5):1026-1034. doi:10.1016/j.mehy.2006.09.051
3. Diederichsen ACP, Lindholt JS, Möller S, et al. Vitamin K2 and D in patients with aortic valve calcification: a randomized double-blinded clinical trial. Circulation. 2022;145(18):1387-1397. doi:10.1161/CIRCULATIONAHA.121.057008
4. De Vriese AS, Caluwé R, Pyfferoen L, et al. Multicenter randomized controlled trial of vitamin K antagonist replacement by rivaroxaban with or without vitamin K2 in hemodialysis patients with atrial fibrillation: the Valkyrie study. J Am Soc Nephrol. 2020;31(1):186-196. doi:10.1681/ASN.2019060579
5. Vossen LM, de Leeuw PW, Schurgers LJ, et al. Two years of menaquinone-7 supplementation and coronary artery calcification: a randomized clinical trial. JAMA Cardiol. Published online 2026. doi:10.1001/jamacardio.2026.1279
6. Kuang X, Liu C, Guo X, Li K, Deng Q, Li D. The combination effect of vitamin K and vitamin D on human bone quality: a meta-analysis of randomized controlled trials. Food Funct. 2020;11(4):3280-3297. doi:10.1039/c9fo03063h
7. Al-Daghri NM, Alkharfy KM, Khan N, et al. Vitamin D supplementation and serum levels of magnesium and selenium in type 2 diabetes mellitus patients: gender dimorphic changes. Int J Vitam Nutr Res. 2014;84(1-2):27-34. doi:10.1024/0300-9831/a000190