The Fastest-Growing Claim in the Category
The creatine-brain connection isn't new. Creatine kinase was mapped in neural tissue in 1993.¹ The first human imaging study confirming that oral creatine could raise brain levels was published in 1999.² The first study to measure a cognitive outcome followed in 2002, with the first cognitive trial using a standard test battery a year later.³ ⁴ For two decades, this was a quiet, niche line of research. Now it's a product category. Major brands are adopting or repositioning creatine with brain-targeted claims. The pitch is simple: the brain demands enormous amounts of ATP, creatine recycles ATP, so more creatine means better cognition. But there's a step the market moved past without resolving. Standard proton MRS, the imaging tool used in nearly every brain creatine study, still can't distinguish creatine from phosphocreatine in a single scan. After thirty years of research, the delivery question is still open. The research tells a different story than the marketing.

Built for Muscle, Sold for Brain
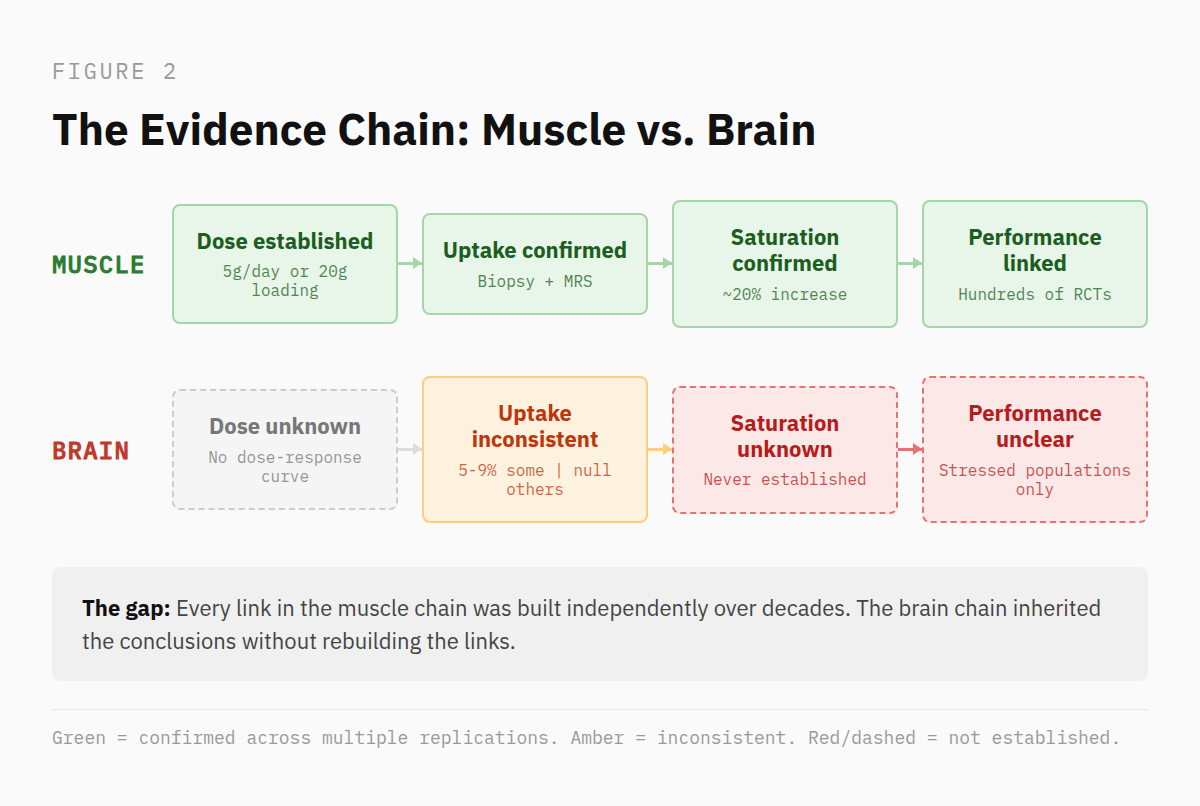
In skeletal muscle, the creatine story is robust and well-defined. Researchers established the dose. They measured uptake. They confirmed saturation. They linked saturation to performance. Every link in that chain has been tested independently and replicated across hundreds of studies.⁵ That chain is what earned creatine its reputation.
The market took the rest from there. When creatine moved into the brain category, the marketing inherited every assumption from muscle (loading protocols, dose ranges, expected timelines) without any of it being validated in neural tissue. The research field did not make that large a leap. Product labels and influencers did.
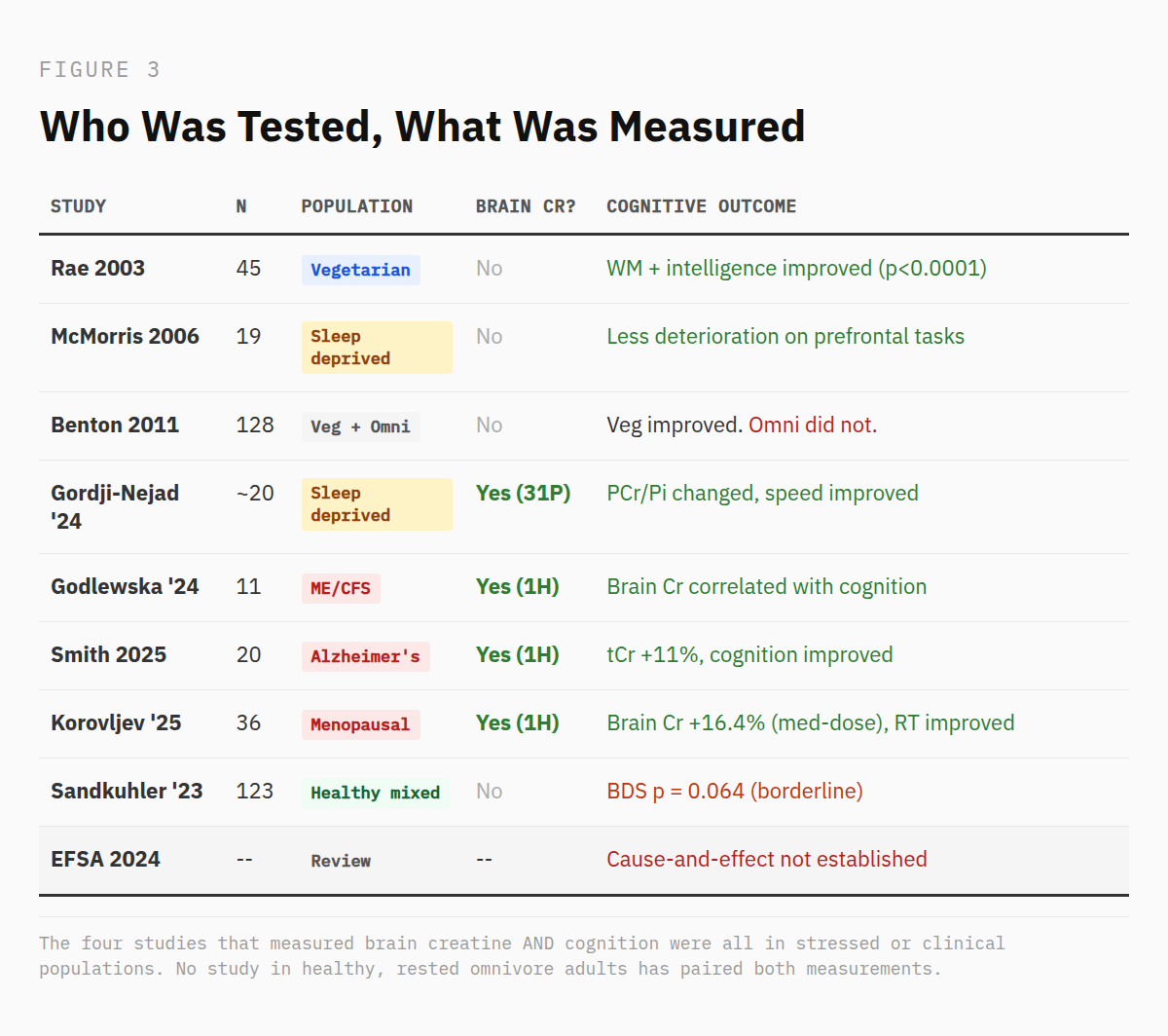
The brain has its own creatine economy. It synthesizes creatine endogenously through a dedicated enzymatic pathway that places real demand on the body's methyl group budget.⁶ It imports creatine from the blood through a dedicated transporter with limited capacity at the blood-brain barrier.7,16 The endogenous synthesis is established. The import pathway is not well-established. And what doesn't exist is the evidence chain connecting oral supplementation to a functional outcome in the brain (bear with me…). No oral dosing protocol has been validated for raising brain creatine to a target concentration. No saturation curve exists. And the link between a measured increase in brain creatine and a corresponding change in cognitive performance has been tested four times: in sleep-deprived healthy adults, in patients with chronic fatigue syndrome, in patients with Alzheimer's disease, and in menopausal women.8-11 Two of those studies included a placebo control. The largest single arm study enrolled twenty people. None tested healthy, rested adults under normal conditions.
A handful of small studies have measured brain creatine after oral supplementation in healthy volunteers. Dechent 1999 found an average 8.7% increase in absolute total creatine concentration in six people after 20 grams per day for four weeks.² Lyoo 2003 found 8 to 9% increases in creatine-to-metabolite ratios in ten men after a two-week loading and maintenance protocol, a directionally consistent finding, though ratios and absolute concentrations are not directly comparable measurements.¹² Pan and Takahashi 2007 found approximately 5% at seven days.¹³ But when Solis 2017 gave a standard loading dose to sixty-four subjects across four populations and measured both muscle and brain, muscle creatine rose 10 to 28%. Brain phosphocreatine barely moved in any group.¹⁴ Same people, same dose, same week. Muscle responded. Brain didn't. Whether that reflects a transport barrier, a limitation of the imaging tools, or both is a question the field has only recently started to confront.¹⁵ ¹⁶ The cognitive trials moved forward anyway.¹⁷
Who Actually Responds
The cognitive data isn't absent. It's patterned. And the pattern doesn't match the marketing.
The trial that launched the brain-creatine category was Rae 2003.⁴ Forty-five subjects took 5 grams per day for six weeks in a crossover design. Working memory and processing speed improved significantly, and the paper (published in Proceedings of the Royal Society B) became the anchor citation for many brain-targeted creatine claims that followed.⁴ What gets cited less often: every subject was vegetarian.⁴ The assumption was that lower dietary creatine intake meant lower brain creatine, and therefore more room for supplementation to help. That assumption has since been tested by imaging. It didn't hold up.¹⁸ But in 2003, nobody checked.
Benton and Donohoe designed a study to test the dietary distinction directly in 2011.¹⁹ One hundred twenty-eight women received 20 grams per day for five days. Vegetarians improved on memory tasks. Omnivores did not.¹⁹ The dietary baseline was thought to determine the response.
The same pattern holds for metabolic stress. McMorris 2006 supplemented subjects with creatine for seven days before 24 hours of sleep deprivation.²⁰ The creatine group showed less deterioration on tasks loading the prefrontal cortex – i.e., random movement generation, choice reaction time, mood.²⁰ Under normal resting conditions, those effects don't appear consistently.
Two meta-analyses have attempted to quantify this. Prokopidis 2023 pooled eight RCTs and found that the age of the subject predicted the result.²¹ Older adults aged 66 to 76 showed a large improvement in memory (SMD = 0.88, P = 0.009). Adults aged 11 to 31 showed no effect (SMD = 0.03, P = 0.72).²¹ Xu 2024 expanded the pool to sixteen RCTs and confirmed a small positive effect on memory overall, but noted the benefit was concentrated in individuals with diseases, in females, and that the certainty of evidence for most cognitive domains was low.²²
The longest creatine-only cognitive trial to date is Sandkuhler 2023.²³ One hundred twenty-three participants, half vegetarian, half omnivore, 5 grams per day for six weeks, crossover design. Working memory improvement bordered statistical significance (P = 0.064) with Bayesian analysis supporting a small effect. Not a null, but not a clear positive either.
In November 2024, the European Food Safety Authority reviewed twenty-three human intervention studies and issued its conclusion: a cause-and-effect relationship has not been established between creatine supplementation and an improvement in cognitive function.²⁴ The acute working memory effect appeared only at 20 grams per day for five to seven days (a loading dose, not a maintenance dose) and was not replicated at lower intakes.
The pattern across three decades of trials is consistent: creatine supplementation shows cognitive effects in populations that are depleted, aged, or metabolically stressed.¹⁵ The young, healthy, well-fed omnivore (the primary target of brain-creatine marketing) is the population with the least evidence of benefit.
The Tools, the Tissue, and the Question Nobody Can Answer
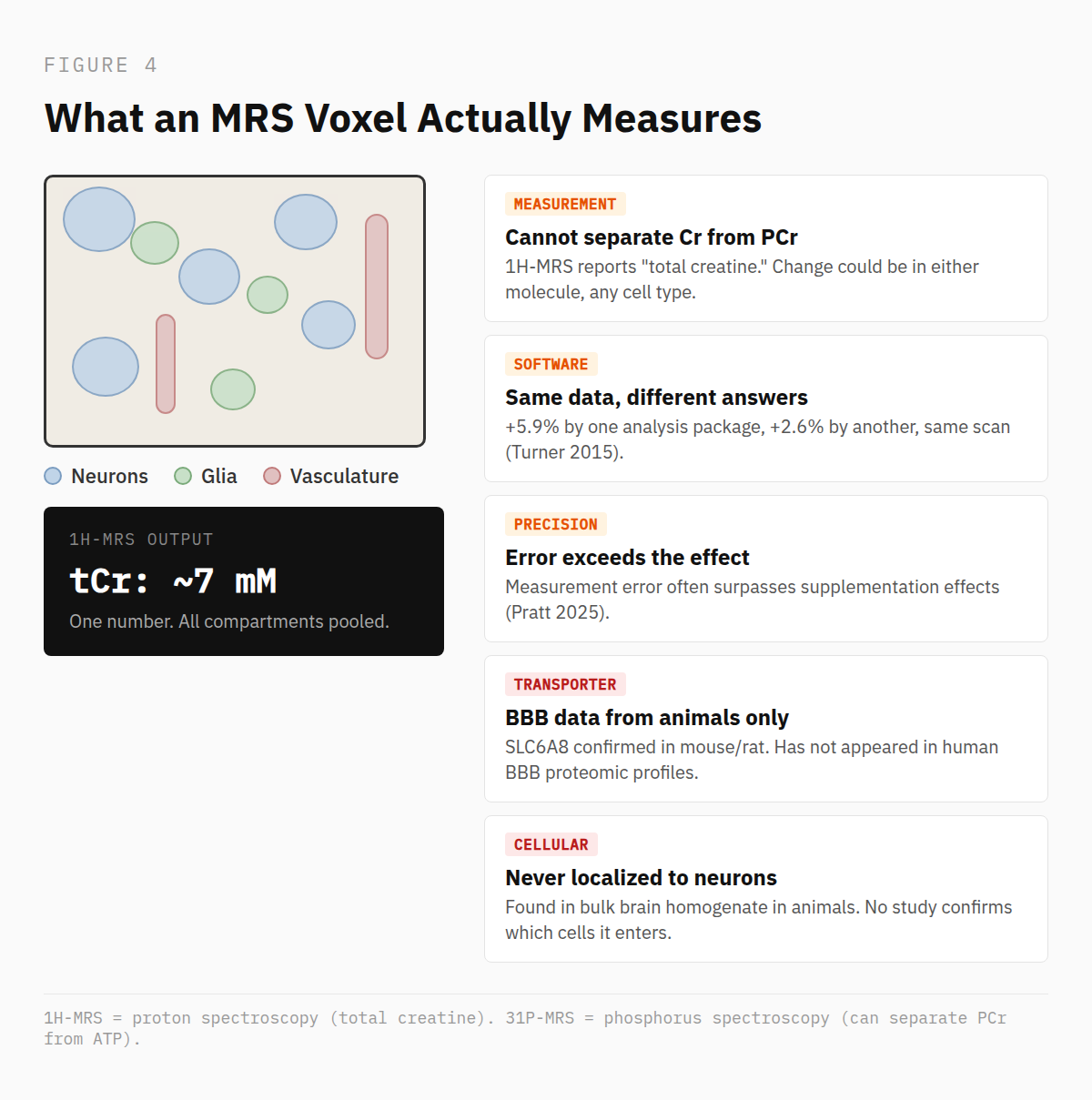
The imaging tool behind nearly every brain creatine claim is proton magnetic resonance spectroscopy (1H-MRS). It reports a composite signal called total creatine from a voxel containing millions of cells (neurons, glia, vasculature, extracellular fluid). It cannot distinguish which compartment the creatine is in.²⁵ And it cannot separate creatine from phosphocreatine. Every "brain creatine increase" measured by 1H-MRS is a pooled signal that could reflect a change in either molecule, in any cell type, in any compartment within the voxel.
The precision of that signal is tighter than its accuracy. Turner 2015 ran the same 1H-MRS supplementation data through two commonly used analysis packages and got two different answers – i.e., a significant 5.9% increase by one method, a non-significant 2.6% by the other.²⁶ Pratt 2025 tested 1H-MRS reliability directly and found that methodological margins of error in repeated scans often surpass the reported effects of supplementation itself.²⁷ Candow 2026 concluded that voxel placement, signal quality, analysis pipelines, and reporting conventions are variable enough across labs to obscure the detection of biological responses to supplementation on 1H-MRS.²⁸
Phosphorus spectroscopy (31P-MRS) can separate phosphocreatine from ATP and inorganic phosphate, which is why Gordji-Nejad 2024 used it to show cerebral phosphate changes during sleep deprivation.⁸ But when Solis 2017 used 31P-MRS to measure brain phosphocreatine after a loading protocol, it did not change.¹⁴ Dechent 1999 found an 8.7% increase using 1H-MRS.² Two different tools measuring two different signals. The field, at times, has treated them as telling the same story. They may not be.
Then there is the transporter. The claim that creatine crosses the blood-brain barrier through SLC6A8 was established in rodent models over two decades ago.29,35 The most recent comprehensive review of creatine transport at the brain barrier, published in 2026, still relies on that same animal foundation.³⁰ The only human-derived data comes from an immortalized cell line, not native tissue.³¹ And SLC6A8 has not appeared in the published quantitative profiles of human BBB transporters.³² Whether orally supplemented creatine enters neural tissue specifically has not been confirmed at the cellular level in any species. Animal studies have measured increased creatine in bulk brain homogenate, but none has localized it to neurons.³³
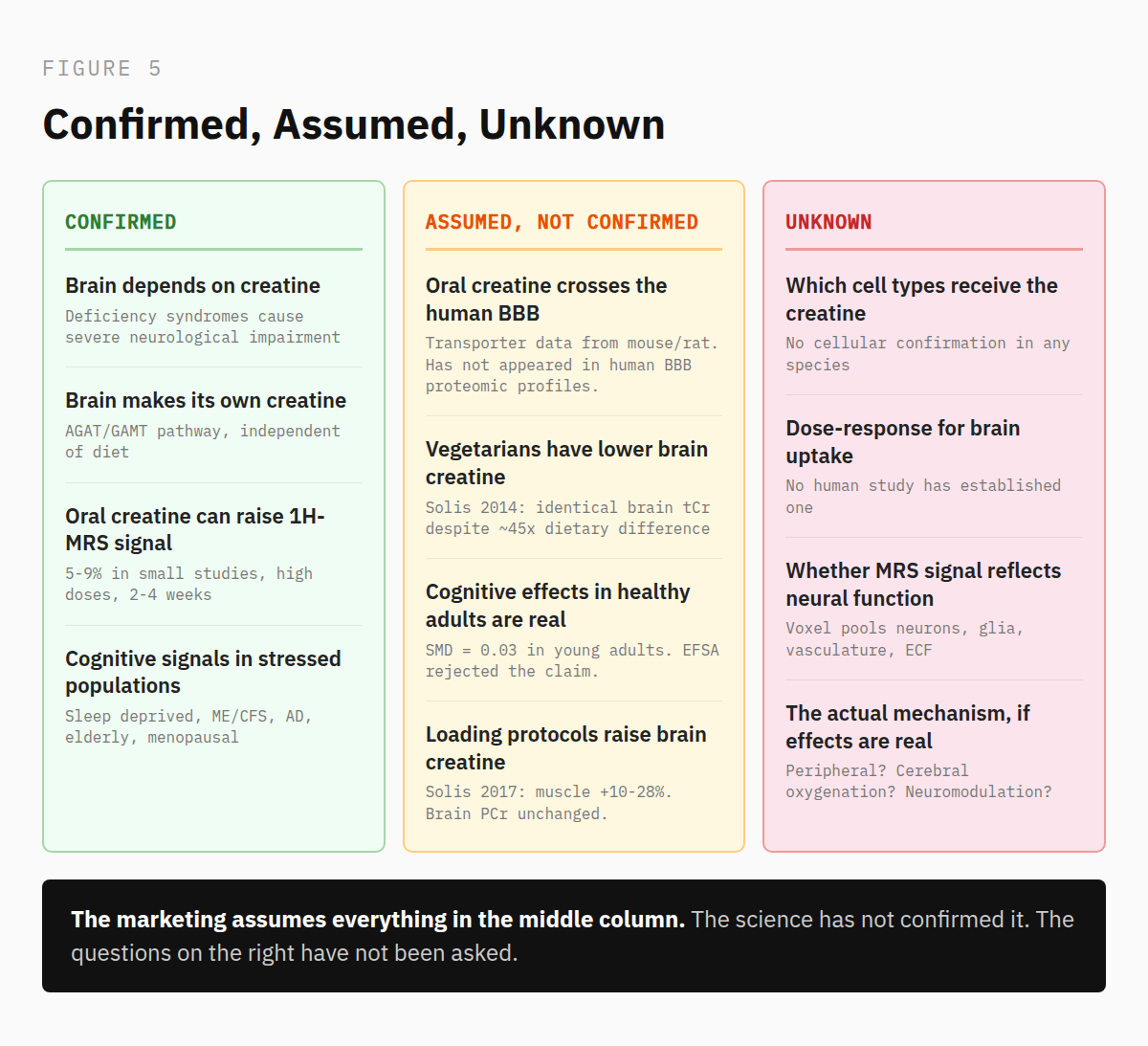
And here is what makes all of this more than a methodological footnote. In small studies of clinically challenged populations, brain creatine does appear to rise after supplementation, and cognitive measures have improved alongside it.8-11 Those signals are preliminary and uncontrolled, but they are directionally consistent. The problem is the other half of the literature. The studies in healthy, rested adults that report cognitive benefits never measured brain creatine.¹⁵ They used heterogeneous doses, durations, and cognitive batteries. They assumed delivery was happening and tested outcomes. Some found effects. Whether those effects are real or artifacts of variable methods and small samples is unresolved. And underneath both stories sits the finding this investigation keeps returning to. Vegetarian brains are not depleted of creatine.¹⁸ A standard loading dose does not reliably raise brain levels.¹⁴ Yet some populations do respond cognitively. If the brain isn't depleted by diet and loading doesn't reliably raise brain levels, the mechanism producing those cognitive effects, if they are real, is unknown. The field assumed the answer was delivery, but it’s possible it may be something else entirely.
What the Evidence Actually Supports
Creatine is essential for brain bioenergetics. Genetic conditions that disrupt creatine synthesis or transport cause severe intellectual disability and seizures, confirming the brain's absolute dependence on this system.³⁴ That was never in question.
What the evidence supports beyond that is narrower than the market suggests. In small studies of clinically compromised populations, oral supplementation does appear to raise brain creatine and improve some cognitive measures. Those findings are preliminary, mostly uncontrolled, and confined to people under metabolic stress. They are worth pursuing. They are not the basis for a product category aimed at healthy adults.
In healthy, rested omnivores, the cognitive signal is weak to absent. The meta-analyses find no effect in young adults.²¹ The most rigorous single trial bordered significance on one measure.²³ The European Food Safety Authority reviewed the full body of evidence and rejected the claim.²⁴ The positive findings that do exist in healthy populations come from studies that never confirmed the creatine reached the brain, used variable methods, and tested outcomes before establishing mechanism.
The usual conclusion here would be that more research is needed. That is true but insufficient. The research that is needed is not another cognitive questionnaire study at five grams per day. The foundational questions are upstream. Can oral creatine cross the human blood-brain barrier in meaningful amounts? Which cell types does it reach? Does the increase measured on MRS reflect a functional change in neural tissue, or a signal from a voxel that cannot tell you where the creatine went? And if certain populations do respond cognitively without confirmed brain delivery, what mechanism is actually responsible?
Until those questions are answered, the marketing claims are running ahead of the science behind it.
References
1. Hemmer W, Wallimann T. Functional aspects of creatine kinase in brain. Dev Neurosci. 1993;15(3-5):249-60.
2. Dechent P, et al. Increase of total creatine in human brain after oral supplementation of creatine-monohydrate. Am J Physiol. 1999;277(3):R698-704.
3. Watanabe A, et al. Effects of creatine on mental fatigue and cerebral hemoglobin oxygenation. Neurosci Res. 2002;42(4):279-85.
4. Rae C, et al. Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. Proc Biol Sci. 2003;270(1529):2147-50.
5. Kreider RB, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14:18.
6. Brosnan JT, Brosnan ME. The metabolic burden of creatine synthesis. Amino Acids. 2011;40(5):1325-31.
7. Snow RJ, Murphy RM. Creatine and the creatine transporter: a review. Mol Cell Biochem. 2001;224(1-2):169-81.
8. Gordji-Nejad A, et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep. 2024;14(1):4937.
9. Godlewska BR, et al. Six-week supplementation with creatine in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a magnetic resonance spectroscopy feasibility study at 3 Tesla. Nutrients. 2024;16(19):3308.
10. Smith AN, et al. Creatine monohydrate pilot in Alzheimer's: feasibility, brain creatine, and cognition. Alzheimers Dement (N Y). 2025;11(2):e70101.
11. Korovljev D, et al. The effects of 8-week creatine hydrochloride and creatine ethyl ester supplementation on cognition, clinical outcomes, and brain creatine levels in perimenopausal and menopausal women (CONCRET-MENOPA): a randomized controlled trial. J Am Nutr Assoc. 2026;45(3):199-210.
12. Lyoo IK, et al. Multinuclear magnetic resonance spectroscopy of high-energy phosphate metabolites in human brain following oral supplementation of creatine-monohydrate. Psychiatry Res. 2003;123(2):87-100.
13. Pan JW, Takahashi K. Cerebral energetic effects of creatine supplementation in humans. Am J Physiol Regul Integr Comp Physiol. 2007;292(4):R1745-50.
14. Solis MY, et al. Effect of age, diet, and tissue type on PCr response to creatine supplementation. J Appl Physiol (1985). 2017;123(2):407-414.
15. McMorris T, et al. Creatine supplementation research fails to support the theoretical basis for an effect on cognition: evidence from a systematic review. Behav Brain Res. 2024;466:114982.
16. Machado M. Creatine supplementation and cognitive aging: the challenge of crossing the blood-brain barrier. Nutr Health. 2025 (online ahead of print).
17. Dolan E, et al. Beyond muscle: the effects of creatine supplementation on brain creatine, cognitive processing, and traumatic brain injury. Eur J Sport Sci. 2019;19(1):1-14.
18. Yazigi Solis M, et al. Brain creatine depletion in vegetarians? A cross-sectional 1H-magnetic resonance spectroscopy (1H-MRS) study. Br J Nutr. 2014;111(7):1272-4.
19. Benton D, Donohoe R. The influence of creatine supplementation on the cognitive functioning of vegetarians and omnivores. Br J Nutr. 2011;105(7):1100-5.
20. McMorris T, et al. Effect of creatine supplementation and sleep deprivation, with mild exercise, on cognitive and psychomotor performance, mood state, and plasma concentrations of catecholamines and cortisol. Psychopharmacology (Berl). 2006;185(1):93-103.
21. Prokopidis K, et al. Effects of creatine supplementation on memory in healthy individuals: a systematic review and meta-analysis of randomized controlled trials. Nutr Rev. 2023;81(4):416-427.
22. Xu C, et al. The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis. Front Nutr. 2024;11:1424972.
23. Sandkuhler JF, et al. The effects of creatine supplementation on cognitive performance — a randomised controlled study. BMC Med. 2023;21(1):440.
24. EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA). Creatine and improvement in cognitive function: evaluation of a health claim pursuant to article 13(5) of regulation (EC) No 1924/2006. EFSA J. 2024;22(11):e9100.
25. Palombo M, et al. Insights into brain microstructure from in vivo DW-MRS. NeuroImage. 2018;182:97-116.
26. Turner CE, et al. Comparative quantification of dietary supplemented neural creatine concentrations with 1H-MRS peak fitting and basis spectrum methods. Magn Reson Imaging. 2015;33(9):1163-1167.
27. Pratt J, et al. Intra- and inter-session reliability and repeatability of 1H magnetic resonance spectroscopy for determining total creatine concentrations in multiple brain regions. Exp Physiol. 2025;110(3):464-477.
28. Candow DG, et al. Creatine supplementation and the brain: have we put the cart before the horse? J Diet Suppl. 2026;23(2):175-204.
29. Ohtsuki S, et al. The blood-brain barrier creatine transporter is a major pathway for supplying creatine to the brain. J Cereb Blood Flow Metab. 2002;22(11):1327-35.
30. Tachikawa M. Transporters for creatine and related guanidino compounds: their relevance to brain health and disorders. Biol Pharm Bull. 2026;49(4):601-617.
31. Uemura T, et al. Cyclocreatine transport by SLC6A8, the creatine transporter, in HEK293 cells, a human blood-brain barrier model cell, and CCDSs patient-derived fibroblasts. Pharm Res. 2020;37(3):61.
32. Uchida Y, et al. Quantitative targeted absolute proteomics of human blood-brain barrier transporters and receptors. J Neurochem. 2011;117(2):333-45.
33. Ipsiroglu OS, et al. Changes of tissue creatine concentrations upon oral supplementation of creatine-monohydrate in various animal species. Life Sci. 2001;69(15):1805-15.
34. Stockler-Ipsiroglu S, van Karnebeek CD. Cerebral creatine deficiencies: a group of treatable intellectual developmental disorders. Semin Neurol. 2014;34(3):350-6.
35.Braissant O, et al. Endogenous synthesis and transport of creatine in the rat brain: an in situ hybridization study. Brain Res Mol Brain Res. 2001;86(1-2):193-201.